
- Diseases of the Heart: 173/100k vs 216/100k per year for Blacks vs Whites
- Cancer: 154/100k vs 199/100K
- Cerebrovascular Diseases: 42/100k vs 47/100k Source
The picture changes considerably if we look at a single slice-in-time. I chose the "slice" from 45-to-54 years of age because those are peak earning years and there are often children still at home.
- Diseases of the Heart: 134/100k vs 72/100k per year for Blacks vs Whites
- Cancer: 114/100k vs 93/100K
- Cerebrovascular Diseases: 25/100k vs 10/100k
One small, mathematical note: The 100k in the divisor refers to the number of people in that ten-year slice-of-time and not to the total population of all age groups. You cannot simply add-up the death-rates when they are age-stratified.
Access to Primary Care Providers
One of the "contrasts" in the last set of numbers is that the ratio between cancer death-rates is not as pronounced as the B:W ratios for heart disease and strokes.
One plausible hypothesis is that Blacks can get healthcare but they cannot get it quickly. That is, Heart and Cerebrovascular disease are fast-moving and require quicker responses than Cancer.
 |
| Detroit, 640k people, 143 square miles and 17 Primary Care outlets according to Google. |
 |
| Livonia, Michigan, 95k people, 36 square miles and 12 "dots" for Primary Care outlets. |
One of my frequent commenters TSgt-Joe used to be a Social Worker in Detroit and in a different post he commented about the difficulty in getting clients to medical appointments. It was not uncommon for a pregnant woman to travel two-hours by bus or ride-share to her appointment. A lot of appointments don't get made when it is that hard to get there.
Another consideration about Heart Attacks and Strokes is that some kinds of elevated-risk can be identified during routine checkups: Inflammation markers like CRP, high blood pressure, lipid-profile, blood-sugar levels, atrial fibrillation and so on.
Why so few Primary Care Providers in the Inner City?
Income tax: Residents pay 2.4% in income tax and non-residents pay 1.2% in Detroit. Other legacy cities also levy income taxes.
Throttled Income: Inner cities have a disproportionate share of Medicaid payments. Medicaid reimbursements are often below the cost-to-provide. PCP in the suburbs have more patients with private insurance to soften the revenue hit.
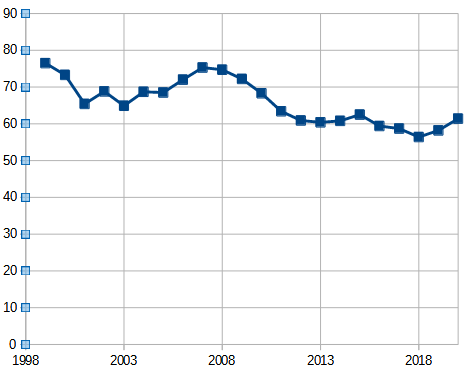
Crime: Detroit has a violent crime rate of approximately 2000/100k per year
Roads: The roads are not well maintained and eat BMWs for lunch. One doctor who I know personally purchased a used Crown Vic in dark blue to be his daily ride to a hospital on the northern fringe of Detroit.
Few amenities: Restaurants? Barber shops? Retail shops? Maybe a few...but not an enjoyable stroll to-and-from away.
Aging facilities and other infrastructure: Not as nice to work in.
Facilities consolidated into massive outlets: Large, fortress-like facilities lack the collegial atmosphere of smaller, more accessible outlets. People don't like working in a place where they have to walk a quarter-mile through a parking lot or parking ramp and pass through two levels of security.
The one thing that could be changed tomorrow would be to remove the income tax on Doctors, Nurse-Practioners, Physician's Assistants, Pharmacists and Registered Nurses.
Another thing that could happen tomorrow would be to investigate and prosecute perps who commit violent crimes that victimize people working in the Primary Care fields more vigorously. That would send a message: Do not mug people in certain parking lots or parking ramps. Do not mug people within a block of a PCP outlet or rob drugstores.
Major roads servicing Primary Care outlets could be fixed over a six-month time-horizon.
The other issues fall under the heading of "Culture" and would be slower to address.
Bonus images
 |
| SIDS plus Accidental Suffocation death-rates per 100k, 1999-2020 |
 |
| Recommended vax for children 1999. You can click on the images to enlarge them. |
 |
| Recommended vax children 2018. |
Incidentally, all US vaccines have been free of thiomersal (mercury) since March, 2001
Part 1: Black-White Mortality Differences
Part 3: IQ? Genetics? Culture?
Saying there is no Thiomerisol in child vaccines is like banning MSG from food in the '80's. They just come up with new names for slight changes. They are using aluminum now instead of mercury.
ReplyDeleteThere are studies done on this! There is a clinic outside of Portland Oregon that has over 20 years of records çompairing vaxxed kids to non Vaxxed kids. The numbers aren't even close. You have a granddaughter. I am not saying all Vaxxes are bad (I would but you would shut down mentally before accepting that.) just wait until she is two.
Ps, the MMR Vaxx is one of the most dangerous for SIDS and autism!
Trumeter: Please back your statement up with data.....real, data, collected in a scientifically and statistically valid method.....if you can .
DeleteOtherwise I call Bullshit.
I think you are just repeating something you heard on Tik-Tok from someone else whose credentials you have no clue about.
Let me lead by saying that Quicksilver (ironically another name for Mercury) has all of her major parenting decisions made by her parents.
DeleteHaving gotten that out of the way, it is very valid to point out that the CDC cadence of vax is probably not based on a typical child's risk.
More likely, they are thinking about the toddler who is shipped to a large daycare (+40 over the course of a week) that is housed in a wing of an elementary school with +400 kids. Many of the kids in the daycare get shipped out to a county-wide program like Head Start. Furthermore, the kiddo has a mother who is likely to get pregnant again. The "R" in "MMR" is for Rubella which causes serious birth-defects.
If you draw the connections and then the connections from the first ring out...the potential for exposure is enormous.
It can be argued that the CDC cadence might be appropriate for THAT kid and that family. It might be gross over-kill for a kid that goes to church once-a-week with her parents and daycare is provided by two of her grandparents.
I am not arguing with you. I am suggesting a different line of logic when you want to convince people.
You will not find scientific studies which establish either the safety or the effectiveness of vaccines, because those studies are never done. Never.
DeleteAnon @ 7:13L If you have the wherewithal to face the truth that disagrees with what you want to believe, read these:
Deletehttps://pmc.ncbi.nlm.nih.gov/articles/PMC2831678/
https://time.com/5175704/andrew-wakefield-vaccine-autism/
And from the Autism people themselves:
https://www.autismspeaks.org/do-vaccines-cause-autism
https://www.autismspeaks.org/science-news/no-mmr-autism-link-large-study-vaccinated-vs-unvaccinated-kids
https://www.autismspeaks.org/science-news/no-association-between-autism-vaccines
Just because you heard from your girlfriends roommate, who heard it from her sister, who got it from her landlord, who heard it from his wife, who got it from her boss, who read it on Facebook doesn't make it true....
Joe: White people living in rural areas have the same issue getting to care (even worse as there is NO public transportation).While accessibility may be a part of the issue, there must be something else also.
ReplyDeleteCrime is likely the biggest factor. Places in Chicago like Rush Presbyterian are in a very bad part of the south side of town, but the immediate area around the health complex is oddly free of crime....so you might have a good idea there.
EXACTLY! The red herring that is sold to the population as "food deserts" is because they ROB EVERY STORE BLIND!
DeleteExample after example of stores moving into bad neighborhoods w/ great fanfare from the politicians only to be shuttered a year or two later, citing theft and employee safety practically every time.
Who's gonna run a pharmacy in the middle of the hood?!?!
Sum dood on da corner
DeleteAnother problem is smaller hospitals and primary care doctors offices are swallowed up by the bigger hospitals. For instance, Greenville Memorial Hospital in another county, 40 miles from us, took over our local hospital, which is six miles away and all doctors and specialists in the immediate area, have to join , or lose hospital privileges.
DeleteAre you in EastTN Mike? I used to service the hospital in Greeneville when I worked at the produce company?
DeleteAbout two hours or so from Greeneville, TN, in the upstate of SC.
DeleteAre we deliberately ignoring the science of genetics and IQ stats in all of this? Or is it an honest oversight?
ReplyDeleteYa know what? Never mind! I will do the honours!
“Shuddup, Filthie!!! GTFO!!!”
It’s all culture, dontchya know!!!
I’ll show myself out…
Genes are a big part of health. I bet Africans in Africa and Africans in America have similar health outcomes.
ReplyDelete